By understanding the history of magnetic therapy, it’s easy to appreciate why and how it’s surrounded in mystery and scepticism. However, this does not negate the fact that promising subsets within magnetic therapy such as Pulsed Electromagnetic Fields (PEMF), Transcranial Magnetic Stimulation (TMS) and gradient modulated magnetic fields like those produced by Q Magnets can provide significant therapeutic benefits. After all, isn’t a large magnet at the leading edge of medical diagnostics? The MRI illustrates the possibilities.
11 out of the 13 randomised controlled trials relevant to multipolar magnets listed on our website, show positive effects over placebo. Some of the studies such as Vallbona, Costantino, Man and Laszlo showed significant pain relieving and fracture healing effects.
The two studies that showed no effect were Collacott and Cepeda.
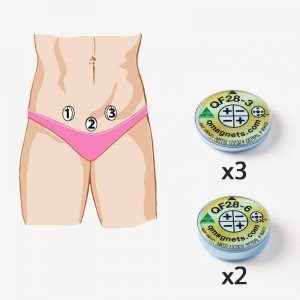
Investigating low back pain was Collacott, who used a weak flexible rubber magnet with an effective penetration of around 10mm. This study was unlikely to show a positive effect because it used the wrong type of magnet. It requires a much more powerful magnet, such as the QF28-6 or OF50-3 to penetrate the 30-40mm required to capture the nerve roots and dorsal horn of the spine to be effective for low back pain.
As for Cepeda, they used a high quality magnet to investigate post operative pain, but placed the devices around the incision. How they could expect a positive result when the field from these magnets did not envelope the target tissue (being the wound), is almost beyond belief.
It is misleading to conclude from these two and other studies, as some observers do that magnetic therapy is not effective. A more scientific conclusion is that the type of magnet used for this condition is not effective. REF
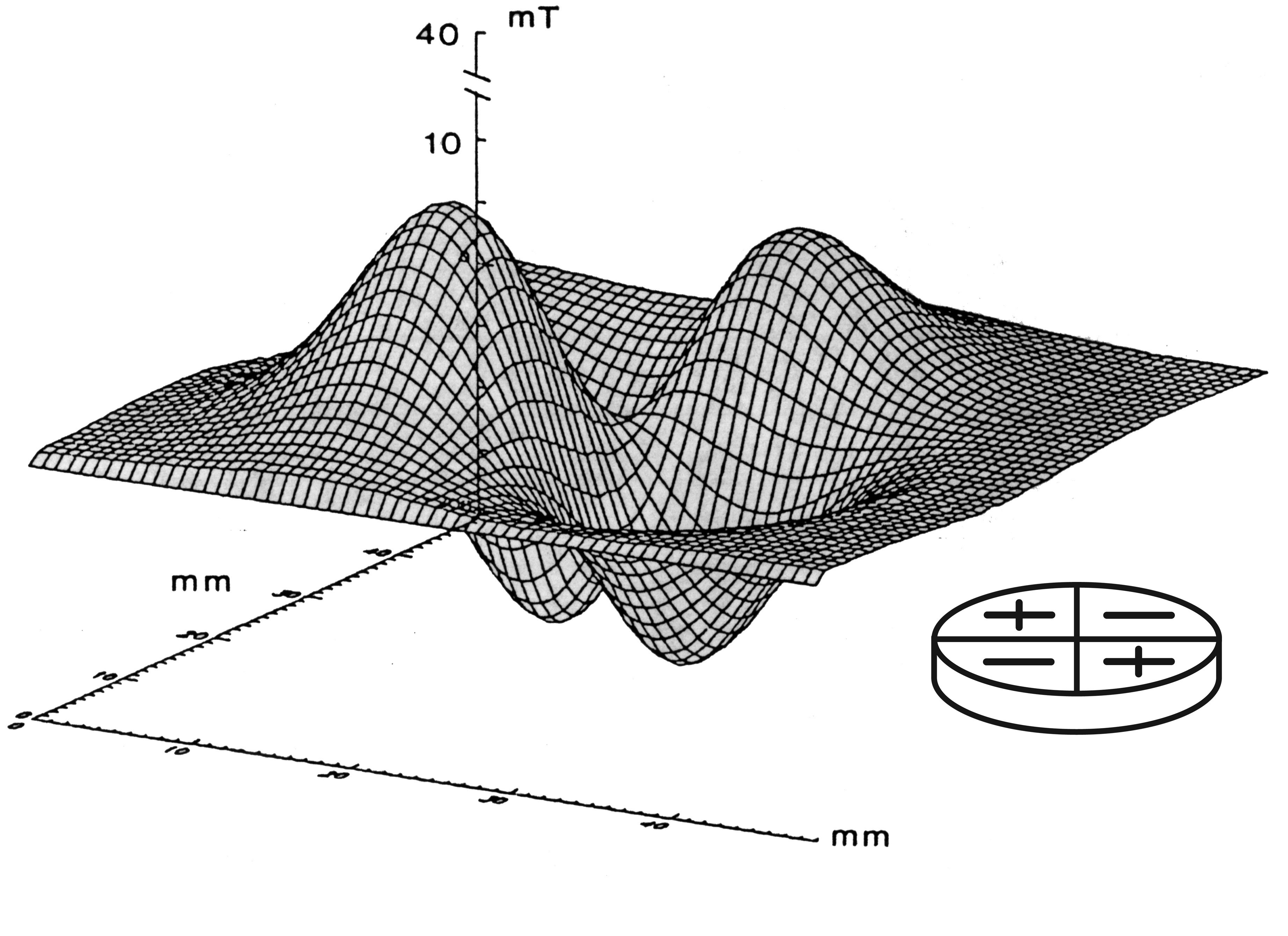
Neuromagnetics is based on the premise that static magnetic fields can be optimised for therapeutic effects and there are ample cell studies, animal studies, case studies and clinical trials to support this.
There appears to be a “window of effectiveness” or therapeutic window for static magnetic devices to produce health benefits. Which is typical of most therapies and should not be suprising. This is where more research needs to be undertaken. We can be thankful that the above two studies help us understand that when the methods operate outside the “window”, then successful clinical outcomes are unlikely.
Just like context-dependant drugs, Q Magnets appear to work on C-fibre nerves in a way that only effects “pathological” pain transmission and not “normal” pain transmission and without the side-effects.
See how Q Magnets effect central sensitization for more information.
Neuro-magnetics
Neuro for the nervous system, being the target of the therapeutic agent, an optimised inhomogeneous magnetic field for modulating pain relief.
Neuromagnetics is recommended to potentially provide comfort or localized temporary relief of minor aches and pains and help people get back to their sport or favourite physical activities sooner. Click on order now, to order your set today.