Scientific evidence for magnetic field therapy
Many people ask, what’s the scientific evidence for using magnets for pain relief?
Like any medical treatment, the subject of evidence should address the question, does it work? But the bottom line is…do the benefits outweigh the risks and inconvenience and justify the costs? The simplicity and low costs of static magnets, certainly sets a low bar in this respect.
For instance, treating conditions such as failed back syndrome with a spinal cord stimulator will cost in the vicinity of $50,000. On top of that, there’s the significant health risks of the surgery itself and ongoing complications and inconvenience for the patient. Yet in many cases, the benefits do outweigh the risks and justify the expense.
Therapies with a risk of serious side-effects and significant expense, understandably require a much greater burden of proof than a treatment with quite the opposite profile. However, not all regulatory bodies see it this way and many will require a high level of evidence to make even mild health claims, regardless of the risks and costs. Which is the reason why as a Class I Medical Device, you see many disclaimers on this website with regard to Q Magnets application.
The hierarchy of evidence pyramid, ranks the strength of evidence; based on study design.

Hierarchy of Evidence Pyramid. Yetley et al (2017). Am J Clin Nutr. Jan; 105(1): 249S–285S.
Expert opinion is the least reliable and case studies are also on the lower end of the quality of evidence spectrum. Nonetheless, case studies can be useful when looking at complex conditions, because they are real clinical cases and patient care should always be based on sound clinical reasoning.
The following studies are organised into 5 categories:
Case Studies
CASE STUDY 1 & 2: ABDOMINAL & GENITAL PAIN
Holcomb et al. (2000) reviewed the cases of two adolescents with medication-resistant chronic pain of the low back and abdomen who had undergone multiple evaluations and interventions by medical specialists. Both cases were treated with multiple alternating quadrapolar array magnet devices made from rare earth magnets. Both were provided rapid relief (within minutes) which was sustained for more than two years.
DISCLAIMER: The safety and effectiveness of Q Magnets has not been established in the treatment of chronic low back and abdominal pain.
Holcomb, R. et al. Static magnetic field therapy for pain in the abdomen and genitals. Pediatr Neurol. 2000;2(3)3:261-4. PMID: 11033291; doi.
Download PDF
CASE STUDY 3: CHRONIC CERVICAL HEADACHES
DISCLAIMER: The case studies by health professionals are not an endorsement of Q Magnets, but for educational purposes only.
CASE STUDY 4: TREATMENT FOLLOWING WHIPLASH
DISCLAIMER: The case studies by health professionals are not an endorsement of Q Magnets, but for educational purposes only.
Case Study 5: 3D Golf Biodyanmic Assessment of Neuromagnetic Treatment
Q Magnets co-founder Dianne Hermans collaborated with University of Iowa to conduct a clinical case study to investigate the short-effects of neuromagnetic treatment on chronic right sacroiliac joint pain of a 35-year-old golf player. 3D gold swing analysis was utilized to complete the procedure. Assessment of the golf swing following application of these devices for 10 min demonstrated an increase in function and range of movement. Increase in hip speed, shoulder speed and hip turn rotation at top of backswing were observed and documented.
Hermans, D. et al. Three-dimensional golf biodynamic assessment of neuromagnetic treatment—A single case study. Journal of Science and Medicine in Sport, Volume 9. 2006. doi
CASE STUDY 6: Knee Pain treatment by a veteran acupuncturist shows the true potential of optimized multipolar magnets in acupuncture
A recent study by a veteran acupuncturist shows the true potential of optimized multipolar magnets in acupuncture and treatment of knee pain:
“..Climbing stairs required 1 step at a time to wait for the pain to subside. Countless consultations with medical specialists that included, physical therapy, acupuncture, pain medication, and other rehabilitation techniques had given him no benefit.
Then I tried magnets. Two octapolar magnets were fastened on the anterior and posterior knee area with adhesive tape. The treatment duration was ∼24 hours. Dramatic results occurred; his pain was completely absent and his limp resolved. His range of motion was normal. This patient could practically run up and down stairs without pain or spasms.
It is now 7 months post-treatment without any signs of relapsing. He continues to ambulate normally and has discontinued all pain medication. The 2 magnets I used, each had a penetration of 35 mm over 1.4 inches and were octapolar (Octapolar OF50-3, Q Magnets..)”
Richard C. Niemtzow.Medical Acupuncture.Apr 2022.81-82. Published in Volume: 34 Issue 2: April 19, 2022. doi
Few More Relevant Case Studies
Panagos, A., et al. Treatment of myofascial shoulder pain in the spinal cord injured population using static magnetic fields: A case series. Spinal Cord Med. 2004
Panagos et al. (2004) in a case series in a university hospital assessed eight participants with myofascial shoulder pain in the spinal cord injured population using inhomogeneous static magnetic fields. The devices used were 500 gauss applied for one hour to the affected shoulder. The magnets were of a flexible concentric field type, measuring 1.5 inches in diameter. The main outcomes were measured using the McGill Pain Questionnaire and pressure algometry were compared. Results using the McGill Pain Questionnaire demonstrated significant decreases in stabbing (p<0.02); sharp (p<0.033); and tender (p<0.021). There was also demonstrated a significant decrease in the present pain intensity (p<0.011). Participants showed a non-significant decrease (p<0.55) on the visual analogue scale and pressure algometry was non-significant (p<0.885).
DISCLAIMER:
The type of magnet used is this study is not a Q Magnet.
The safety and effectiveness of Q Magnets has not been established in the treatment of myofascial shoulder pain.
Panagos, A., et al. (2004). Treatment of myofascial shoulder pain in the spinal cord injured population using static magnetic fields: A case series. Spinal Cord Med. 2004;27:138-142. PMID: 15162885
McDonald, F. “Effect of therapeutic magnets on sympathetic nervous system outflow and pain related measures. Not published. 2004
McDonald, F in a study as part of an BPhty (Hons) degree at Griffith University, conducted a placebo controlled trial on an individual with lateral epicondylalgia. Pain free grip strength (PFGS) and pain pressure threshold (PPT) were used to indicate localised analgesic effects. The PFGS decreased by 18.1% and 6.5% in the control and placebo conditions respectively, but increased by 40% while wearing the active quadrapolar magnet. PPT measured at the elbow decreased by 45.3% and 19.7% from baseline to post intervention periods in the control and placebo conditions respectively (indicative of hyperalgesia) but showed a 26% increase while wearing the active magnet (indicative of analgesia).
The study concluded that there is some evidence for localised analgesic effects suggesting that a local mechanism may be responsible and that the effects observed by the application of quadrapolar magnets cannot be attributed to a placebo effect.
DISCLAIMER:
The safety and effectiveness of Q Magnets has not been established in the treatment of lateral epicondylitis.
Randomised Clinical Trials
Many clinical trials have shown health benefits using magnets. Even for magnetic mattress pads, single bipolar magnets for pain and magnetic bracelets, see the following…
- Magnetic mattress pad in a randomised double-blind pilot study on patients with fibromyalgia. By Colbert et al (1999)
- Static magnet used in a double-blinded, placebo-controlled pilot study to relieve menstrual pain. By Eccles (2005)
- Magnetic bracelets used in a randomised clinical trial to relieve osteoarthritis of the hip and Harlow et al (2004)
Looking through the research, there is a clear pattern. The clinical trials that show a therapeutic benefit, reside predominantly in the studies using multipolar magnets, such as quadrapolar and alternating pole concentric rings.
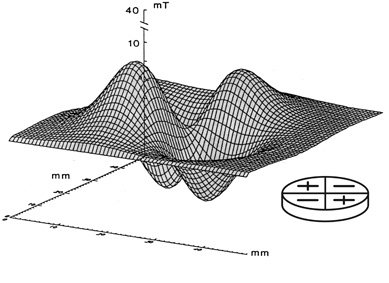
Iron filings showing magnetic field lines on Quadrapolar versus Bipolar magnet


CLINICAL TRIAL 1: QUADRAPOLAR MAGNETS TO TREAT WRIST FRACTURE
Costantino et al. (2007) studied 40 patients with wrist fractures after applying a Quadrapolar array of 12,500 Gauss magnets in the plaster cast directly over the fracture site. Resulting in bone callus formation that produced a 35% improvement in healing rates compared to ‘standard’ time.
DISCLAIMER: The safety and effectiveness of Q Magnets has not been established in the treatment of fractures.
Costantino C., et al. (2007). Treatment of wrist and hand fractures with natural magnets: preliminary report. Acta Bio Medica. 2007;78:198-203; PMID: 18330079.
CLINICAL TRIAL 2 & 3: CONCENTRIC RING MAGNETS TO TREAT TRIGGER POINT PAIN.
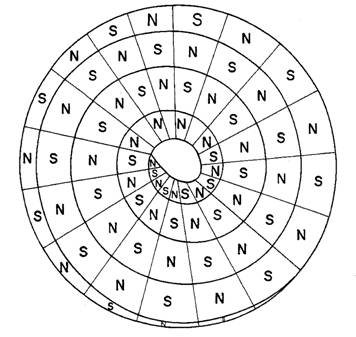
Vallbona et al. (1997) studied 50 patients diagnosed with post-polio syndrome who reported muscular or arthritic-like pain. The double-blind randomized clinical trial applied (300 to 500 Gauss) magnetic devices to the affected area for 45 minutes. The magnets used in this study were a multipolar magnet with concentrically arranged circles of alternating magnet polarity.
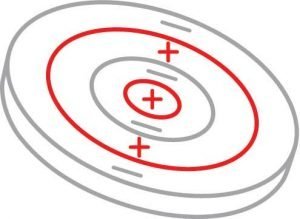
Concentric Rings Alternating Poles
DISCLAIMER: The type of magnet used is this study was not a Q Magnet. The safety and effectiveness of Q Magnets has not been established in the treatment of post-polio pain.
Outcome measures were scored using the McGill Pain Questionnaire. Results of the study using the 10-point scale as follows…
Placebo group – experienced a decrease of pain of 1.1 ± 1.6 points (p<0.005)
Active group – experienced a decrease of pain of 5.2 ± 3.2 (p<0.0001).
Those who received the active device reported much less pain than those who had the inactive device.
Vallbona concluded the application of a static magnetic field of 300-500 Gauss over a trigger point offers significant and prompt relief of trigger point pain in post-polio subjects.
Vallbona C., Hazelwood C.F., et al. (1997). Response of pain to static magnetic fields in postpolio patients: a double-blind pilot study. Arch Phys Med Rehabil. 1997;78(11):1200-3. PMID: 9365349; doi.
Download PDF
The same type of alternating concentric ring magnets were used in a randomised clinical trial with 30 subjects at the Armstrong Atlantic State University Physical Therapy department. The results were not peer reviewed and published, but were presented at a conference, details here.
Obviously not all studies show that magnetic field therapy has a therapeutic benefit. But it’s misleading to make blanket statements based on a specific study to say… “magnetic field therapy does not work”. Such studies can in fact be very useful in learning what works and what doesn’t and why.
For instance, the following clinical trial by Cepeda (see Clinical Trial #4 below), concluded that…
“In summary, bipolar static magnetic therapy lacks efficacy, and its use is not recommended for acute pain relief.”
A more accurate conclusion would have been…
“In summary, placing the type of static magnet used in this study around a surgical wound lacks efficacy, and is not recommended for acute pain relief.”
After all, I doubt the same researchers would inject a local anaesthetic into the elbow joint and from that deduce it lacks efficacy for knee pain. Other studies, such as by Man, D., et al. (1999) did place the magnet directly over the surgery site and did show a benefit.
Although this study could be perceived as negative, it is still very useful. The lesson learned is that poor placement will produce poor outcomes.
CLINICAL TRIAL 4: EFFECT OF MAGNETIC THERAPY ON POSTOPERATIVE PAIN.
Cepeda et al. (2007) used quadrapolar static magnets for this study, but unfortunately did not place the magnets over the wound. Health professionals experienced with using quadrapolar magnets know that after surgery, you place the magnets directly over the wound incision, over the dressing of course. The image below shows where the magnets were applied for this study.

Positioning of magnets in Cepeda study around the surgical incision. Any wonder there was no effect!
In fact, very few are even close to the recommended treatment protocol for abdominal pain.
Unlike systemic drugs used by anesthetists, the physiological effect of magnets is very specific and localised. The intensity of a static magnetic field diminishes in proportion to the inverse of the cube of the distance. Correct placement of Q Magnets to effect nerve tissue, pain and inflammation is vital in order to achieve pain relief or injury recovery. Placements out by as little as 1 cm or ½ inch can make all the difference.
This study was never going to achieve a successful outcome for magnetic therapy because of its poor design.
Cepeda, M., et al (2007). Static Magnetic Therapy does not decrease pain or opioid requirements: A randomized double-blind trial. Anesth & Analg 2007;104:290-294. PMID: 17242082; doi
For different reasons, the following clinical trial by Collacott concluded that the type of permanent magnet used in the study, had no effect on chronic low back pain. At least the authors were intelligent enough to make the following qualifications…
A stronger magnet may be necessary to penetrate to the source of chronic low back pain.
Our results did not support the findings of Vallbona and Weintraub. However, there were considerable differences in the study designs and populations, including the cause of pain. The patients of Vallbona and colleagues had muscle pain while Weintraub’s subjects had neuropathic pain. The source of pain in our participants would appear to be deeper than that of the former, and may explain the lack of beneficial effect from the magnets used (300 G).
Although this study could be perceived as negative, it is still very useful. The main lesson learned is that poor selection of magnetic device will produce poor outcomes.
CLINICAL TRIAL 5: EFFECT OF MAGNETIC THERAPY ON CHRONIC LOW BACK PAIN
Collacott et al. (2000) was a randomized, double blind, placebo-controlled crossover pilot study with a sample of 20 subjects with chronic degenerative low back pain. The active multipolar magnet with 30 mT (300 Gauss) was worn for six hours per day for three days per week for one week for a total of 18 hours for both demagnetized sham and magnetic devices.
The multipolar arrangement of the magnetic device can be seen from the manufacture’s (Nikken) 1996 patent # 5,538,495.

The Japanese Company; Nikken Magnets
An amusing perspective with this study is how often it is quoted by sceptics as proof that magnetic therapy does not work. However, the 300 G magnets used would barely penetrate 12 mm (1/2 inch), which when considering the spinal cord at the lower back level is closer to 50 mm (2 inches) away from the skin’s surface would explain why this study proved no efficacy.
Collacott, E.A., Zimmerman, J.T., et al. (2000). Bipolar permanent magnets for the treatment of chronic low back pain. JAMA. 2000;283(10):1322-5. PMID: 10714732; doi.
A more scientific response to the two studies above is described by Colbert, that is, the type of magnet used for the condition treated did not show a therapeutic benefit.
There is so much misleading information out there with regard to static magnets. For instance, the statements put out by government organisations such as the US National Center for Complementary and Integrative Health do not even mention the more promising areas of research. They have since shortened their fact sheet, but the previous one is still available for download on our website. Our response to the misinformation on the fact-sheet can be found here.
CLINICAL TRIAL #6: QUADRAPOLAR MAGNETS TO TREAT RHEUMATOID ARTHRITIS OF THE KNEE
Segal et al. (2001) studied 64 patients with Rheumatoid Arthritis who suffered moderate knee pain by application of four 190 mT (1900 Gauss) quadrapolar magnets in one group and in a placebo group with a weak standard bipolar magnet with a homogeneous field of strength 72 mT (720 Gauss).
DISCLAIMER: The safety and effectiveness of Q Magnets has not been established in the treatment of rheumatoid arthritis.
Subjects randomly assigned to the quadrapolar magnet group showed a greater reduction in joint pain than did the control group after one week follow up (40.4% vs 25.9%) and twice daily pain diary results (p< 0.0001) for each vs baseline.
However, comparison between the two groups demonstrated no statistical significance (p<.23). Subjects in the quadrapolar magnet group reported an average decrease in the global assessment of the disease activity of 33% over one week, as compared with a 2% decline in the control group (p<0.01).
After one week, 68% of the quadrapolar magnet treatment group reported feeling better compared with 27% of the control group. Whilst 29% of the active group and 65% of the placebo group reported feeling the same as before treatment (p<0.01). Segal concluded that both devices demonstrated statistically significant pain reduction compared to baseline. However, a significant difference was not observed between the two treatment groups (p<0.23).
Segal recommended that a nonmagnetic placebo treatment be used to further characterize its therapeutic potential for treating rheumatoid arthritis. Randomised controlled clinical trials are difficult to control for with static magnets. Protecting the blind in clinical trials that run for days or weeks is difficult, because subjects can somewhat easily test the magnet at home with something metal. Segal’s study used a weak placebo as a workaround, but the question is, is this a true placebo or does it become a dose comparison study.
Segal, N.A., Toda, Y., et al. (2001). Two configurations of static magnetic fields for treating rheumatoid arthritis of the knee: a double-blind clinical trial. Arch Phys Med Rehabil: 2001 Oct;82(10):1453-60;. PMID: 11588753; doi.
Download PDF
CLINICAL TRIAL #7: QUADRAPOLAR MAGNETS TO TREAT LOWER BACK PAIN.
Holcomb et al. (1991) in a multi-centre randomized crossover study on 54 subjects with low back or knee pain. The placebo was non-magnetic and the active device was an in-homogeneous 200 mT (2000 G) quadrapolar array.
The magnetic devices were worn for 24 hours with a seven day washout period. Holcomb reported a significant reduction in low back and knee pain at 1 and 24 hours but not at 3 hours.
Unfortunately this article has not been peer reviewed and efficacy of blinding and low subject numbers are questioned along with heterogeneity of diagnosis (some subjects had both back and knee pain).
Holcomb RR, Parker RA, Harrison MS. Biomagnetics in the treatment of human pain-past, present, future. Environ Med. 1991;8:24-30.
Download PDF
What about using the north or south pole of a magnet? Some people think that’s the critical thing about using magnetic therapy, except when you look at the published research, it seems to be saying it makes no difference. See the article – Is there any difference to using the north or south pole of a magnet to learn about rationale and evidence for which magnet to use.
Few More Relevant Randomized Clinical Trials:
Kovacs-Balint, Z., Csatho, A., et al. (2011). “Exposure to an inhomogeneous static magnetic field increases thermal pain threshold in healthy human volunteers.” Bioelectromagnetics 2011
Kovacs-Balint et al. (2011) used previous research with animal studies such as Laszlo et al (2007) and Sandor et al, (2007) on optimized inhomogeneous static magnetic fields to induce analgesia. A similar inhomogeneous static magnetic field (iSMF) was used to investigate the attenuating effects of iSMF on the thermal pain threshold (TPT) in healthy young adults in a double-blind, placebo controlled manner.
The finger tips of 15 healthy subjects were exposed to the iSMF with a maximum gradient of 13.2 T/m for 30 minutes. TPT and VAS data were recorded at 0, 15 and 30min exposure time. There were three blocks, iSMF, sham and the control and after each block subjects used the VAS to rate the pain. It was demonstrated that exposure to iSMF significantly increases pain threshold (measured in °C). VAS profiles indicated an ongoing increase in pain ratings between measurement blocks in the sham condition, while remaining at a constant level in the genuine condition. Kovacs-Balint, Z., Csatho, A., et al. (2011). “Exposure to an inhomogeneous static magnetic field increases thermal pain threshold in healthy human volunteers.” Bioelectromagnetics 2011;32(2): 131-139. PMID: 21225890; doi.Laszlo, J., et al. Effect of local exposure to inhomogeneous static magnetic field on stomatological pain sensation – a double-blind, randomized, placebo-controlled study. Int J Radiat Biol. 2012
Laszlo et al. (2012) studied 79 adult patients with temporomandibular disorders, alveolitis and aphtha in a randomised controled trial. The active static magnet arrangement produced and inhomogeneous magnetic field with a 0-192 mT peak to peak induction with a 19 T/m lateral gradient at 3mm from the magnet.
Static magnetic field exposure of the active group significantly reduced pain perception (reduction from baseline to post-treatment VAS score) in the group with temporomandibular disorders from 2.0 ± 0.3 versus 0.5 ± 0.1 (n = 29, p = 0.0003. Laszlo, J., et al. (2012). “Effect of local exposure to inhomogeneous static magnetic field on stomatological pain sensation – a double-blind, randomized, placebo-controlled study.”Int J Radiat Biol. 2012 Feb 28 PMID: 22288770; doi.Hermans et al. A pilot trial investigating the effect and effect mechanisms of neuromagnetics treatment on osteoarthritis of the knee. 2011
Hermans et al. (2011) conducted a pilot trial investigating the effect and effect mechanisms of neuromagnetics treatment i.e. an inhomogeneous static magnetic field, on osteoarthritis of the knee. This was a pilot RCT with 5 subjects completing the trial.
DISCLAIMER:
The safety and effectiveness of Q Magnets has not been established in the treatment of osteoarthritis of the knee.
The aim of this study was to examine how the quadrapolar magnets modified the pain response in osteoarthritis of the knee. Although the participant numbers were small, the results demonstrated that there was a non significant downward trend in VAS pain scores as recorded in the participant’s pain diaries.
Quadrapolar rating The active device was a Quadrapolar magnet with internal gauss rating of 13,500 Gauss and equivalent to the QF28-6. Patients were randomly assigned to a week of treatment with an active device or a week with the non-active placebo (control). After the first week, there was a one week washout with no device and then a week with the alternative treatment. Hence a subject starting with one week of the active device, would then have a week break with no device and then a week with the placebo device and vice versa.
Sympathetic nervous system (SNS) pathways such as skin temperature, blood flux and skin conductance were measured immediately before and after application of the devices. Pain scores were measured using WOMAC, the functional squat and VAS (Visual Analogue Scale pain scores) were recorded in a pain diary.
There was no statistical difference in SNS measures between the groups. The descending inhibitory system (through the SNS) is unlikely to be involved in the mechanism of pain relief mediated by static magnetic fields.
The following graph illustrates the mean pain per day for all participants as recorded in a pain diary. There was an upward trend in pain scores during the washout period and improved pain scores were greater with the active magnets than for placebo.

The trial provided evidence suggesting that further research is warranted with greater participant numbers. Yet to be published.
Weintraub, M.I., Wolfe, G.I., et al. Static magnetic field therapy for symptomatic diabetic neuropathy: a randomized, double-blind, placebo-controlled trial.” Arch Phys Med Rehabil. 2003
Weintraub et al. (2003) conducted a multicentre (48 centres in 27 USA states) to assess if 450 gauss multipolar insoles could affect the pain of diabetic peripheral neuropathy. The field generated by the insoles was inhomogeneous as can be seen from the manufactures (Nikken) 1999 patent # 5,871,438.
DISCLAIMER:
The type of magnet used is this study is not a Q Magnet.
The safety and effectiveness of Q Magnets has not been established in the treatment of diabetic peripheral neuropathy.

375 subjects were recruited with symptomatic bilateral sensory and motor neuropathy who were randomly selected to wear either the magnetic or placebo insoles for 4 months (24 hours per day). Symptoms had to be constant and present for at least 6 months and to be 6 months without pain medications.
On assessment of bias and masking there was no significant association between the actual treatment and the placebo from both subjects and investigators. There was significant difference in the third and fourth month in burning, (mean change for magnet treatment, -12%; for sham, -3%; p<0.05 ANCOVA) numbness and tingling, (magnet,-10%; sham, +1%; p<0.05 ANCOVA) and exercise induced foot pain (Magnet, -12%; sham, -4%; p<0.05, ANCOVA).
Weintraub et al (2003) with a subset of patients with baseline severe pain, statistically significant reductions occurred from baseline through the fourth month in numbness and tingling (magnet, -32%; sham, -14%; p< 0.01 ANOVA). Weintraub et al (2003) concluded that static magnetic fields can penetrate up to 20 mm and appear to target the ectopic firing nociceptors in the dermis and epidermis. Over time it is recommended by Weintraub et al (2003) that analgesic benefits occur.
In a study published in JAMA, Collacott used a similar but slightly weaker rubber magnet for the treatment of lower back pain but the lack of depth of penetration was most likely the determining factor in the poor outcomes achieved.
Weintraub, M.I., Wolfe, G.I., et al. (2003). “Static magnetic field therapy for symptomatic diabetic neuropathy: a randomized, double-blind, placebo-controlled trial.” Arch Phys Med Rehabil. 2003;84(5):736-46. PMID: 12736891; doi.
Download PDF
Weintraub, M.I., et al. Magnetic Bio-Stimulation in painful diabetic peripheral neuropathy: a novel intervention – a randomized, double-placebo, crossover study. American Journal of Pain Management. 1999
Weintraub et al. (1999) in a randomized double- placebo, crossover study assessed 19 subjects using 475 gauss inhomogeneous insoles using a sham and active magnets. The field generated by the insoles was inhomogeneous as can be seen from the manufactures (Nikken) 1996 patent # 5,538,495.
DISCLAIMER:
The type of magnet used is this study is not a Q Magnet.
The safety and effectiveness of Q Magnets has not been established in the treatment of diabetic peripheral neuropathy.
The devices were worn for 24 hours per day for 30 days for each phase of trial with a total treatment time of 12 weeks. Weintraub et al (1999) significantly reduced burning pain, tingling and numbness in diabetic group using VAS as measurements.
The limitations of the trial was a lack of double blind component, small size; heterogeneity of subject diagnoses and no wash out period between active and sham episodes.
Weintraub, M.I., et al. (1999). Magnetic Bio-Stimulation in painful diabetic peripheral neuropathy: a novel intervention – a randomized, double-placebo, crossover study. American Journal of Pain Management. 1999;9:8-17.
Brown, C.S., Ling, F.W., Wan, J.Y., et al. (2002). Efficacy of static magnetic field therapy in chronic pelvic pain: a double-blind pilot study. Am J Obstet Gynecol 2002
Brown et al. (2002) studied 32 patients with Chronic Pelvic Pain by measuring pain relief and disability over two weeks and 19 patients completed 4 weeks of randomized double-blind placebo-controlled treatment at a gynaecology clinic. Assessment was made using McGill Pain Questionnaire, Pain Disability Index and Clinical Global Impressions Scale were outcome measures.
DISCLAIMER:
The type of magnet used is this study is not a Q Magnet.
The safety and effectiveness of Q Magnets has not been established in the treatment of chronic pelvic pain.
The results of patients receiving active in homogeneous (500 gauss) or sham placebo magnets were applied to abdominal trigger points for 24 hours per day. From a description of the active devices with a concentric bipolar configuration and the manufacturer’s 1985 patent number 4,549,532, the field patterns were orientated as in the following diagram.

The patients receiving the active magnets who completed four weeks of double-blind treatment had significantly lower Pain Disability Index (p<0.05), Clinical Global Impressions – Severity (p<0.05) and Clinical Global impressions – Improvement (p<0.01) scores than those receiving placebo magnets, yet were more likely to correctly identify their treatment (p<0.05).
Brown et al (2002) concluded that Static Magnetic Field (SMF) therapy significantly improves disability and may reduce pain when active magnets are worn continuously for four weeks in patients with Chronic Pelvic Pain.
Brown, C.S., Ling, F.W., Wan, J.Y., et al. (2002). Efficacy of static magnetic field therapy in chronic pelvic pain: a double-blind pilot study. Am J Obstet Gynecol 2002;187:1581-7. PMID: 12501067; doi.
Man, D., et al. The influence of permanent magnetic field therapy on wound healing in suction lipectomy patients: a double-blind study. Plast Reconstr Surg Dec 1999
Man et al. (1999) randomly assingned 10 patients to an active magnet group and 10 to a placebo group to assess the effects of a permanent static magnetic field on wound healing after liposuction.
DISCLAIMER:
The type of magnet used is this study is not a Q Magnet.
The safety and effectiveness of Q Magnets has not been established in the tfield of wound healing.
The magnet is not well described other than there were multiple ceramic magnets inserted into patches such that the surface strength was between 150 and 400 gauss (15-40 mT) all orrientated with the negative pole to the body.
The results showed that the treatment group had significant reductions in pain on postoperative days 1 through 7, in edema on days 1 through 4 and discolouration on days 1 through 3 when compared to the contol group.
The study concluded that the magnetic field from the active magnet group was quite remarkable in both the prevention and treatment of these signs and symptoms and also in the alleviation of pain itself. The magnitute of the reduction in postoperartive pain was quite significant, allowing for a decrease in the need for analgesic medication. For a more comprehensive review see recover faster from soft tissue injuries.
Man, D., et al. (1999). The influence of permanent magnetic field therapy on wound healing in suction lipectomy patients: a double-blind study. Plast Reconstr Surg Dec;104(7):2261-6. PMID: 11149796; doi.
Juhasz, M., et al. Influence of inhomogeneous static magnetic field-exposure on patients with erosive gastritis: a randomized, self- and placebo-controlled, double-blind, single centre, pilot study. J R Soc Interface. 2014
Juhasz et al. (2014). Sixteen subjects were randomly divided to a placebo/sham group (7) or an active magnet group (9). Researchers wanted to see if the device, placed over the lower sternum for 30 minutes, would significantly contribute to the subjective healing process.
DISCLAIMER:
The type of magnet used is this study is not a Q Magnet.
The safety and effectiveness of Q Magnets has not been established in the treatment of erosive gastritis.
Before and after assessment showed significant benefits over placebo for the symptoms of lower heartburn, regurgitation and bloating.
 Previous studies in mouse models have demonstrated a beneficial effect on symptoms related to inflammation and wound healing beyond that of placebo. It is suspected that the beneficial effect of this magnet on erosive gastritis was due to one or more of the following…
Previous studies in mouse models have demonstrated a beneficial effect on symptoms related to inflammation and wound healing beyond that of placebo. It is suspected that the beneficial effect of this magnet on erosive gastritis was due to one or more of the following…
- Wound healing
- Reinforcing microcirculation of the gastric mucosa
- Endocrine or nitric oxide system balancing
- Direct anti-inflammatory action
Juhasz, M., et al. (2014). Influence of inhomogeneous static magnetic field-exposure on patients with erosive gastritis: a randomized, self- and placebo-controlled, double-blind, single centre, pilot study. J R Soc Interface. 2014 Sep 6;11(98) PMID: 25008086;
Reviews
Laakso et al. (2009). Static Magnets – What are they and what do they do.Brazilian Journal of Physiotherapy: 2009;13(1):10-23.doi. The published article by Laakso (2009) provides the most recent and useful review into static magnets and explains the differences between quadrapolar and bipolar magnets. The article can be downloaded here. Another review by Pittler (2007) published in the British Medical Journal is often quoted and some of the differences between it and Laakso are explained here. Almost all other reviews, including NICCH display such a poor understanding of the science, some of the most important aspects do not even rate a mention. Laakso’s review concludes…In a review of the known literature presented herein, it is not yet clear if static magnets have a significant role to play in the effective management of neuromusculoskeletal pain although some of the research is encouraging.McLean et al. (2001). Static Magnetic Fields for the Treatment of Pain. Epilepsy & Behavior2: S74-S80 (2001).doi. Colbert et al. (2009) Static Magnetic Field Therapy: A Critical Review of Treatment Parameters. Evid Based Complement Alternat Med: 6(2): 133-139. PMID 18955243. doi. Pittler et al. (2007) Static magnets for reducing pain: systematic review and meta-analysis of randomized trials. CMAJ: 2007 Sep 25;177(7):736-42. PMID: 17893349; doi.
Animal Studies
Jaberi et al. (2011). A moderate-intensity static magnetic field enhances repair of cartilage damage in rabbits. Arch Med Res: 2011; 42(4): 268-273. PMID: 21820604; doi. Reference Article
Antal et al. (2009) Exposure to Inhomogeneous Static Magnetic Field Ceases Mechanical Allodynia in Neuropathic Pain in Mice. Bioelectromagnetics: 2009 Sep;30(6):438-45. PMID: 19405037; doi.
Laszlo et al. (2007) Optimization of static magnetic field parameters improves analgesic effect in mice. Bioelectromagnetics 2007 Dec;28(8):615-27. PMID: 17654477; doi.
Laszlo et al. (2009) 3 T homogeneous static magnetic field of a clinical MR significantly inhibits pain in mice. Life Sciences: 2009 Jan 2;84(1-2):12-7. PMID: 19000698; doi.
Morris et al. (2008) Acute Exposure to a Moderate Strength Static Magnetic Field Reduces Edema Formation In Rats. Am J Physiol Heart Circ Physiol: 2008 Jan;294(1):H50-7. PMID: 17982018; doi.
Morris et al (2007). Chronic static magnetic field exposure alters microvessel enlargement resulting from surgical intervention. J Appl Physiol : 2007 Aug;103(2):629-36. PMID: 17478604; doi.
McLean et al. (2003)A static magnetic field modulates severity of audiogenic seizures and anticonvulsant effects of phenytoin in DBA/2 mice. Epilepsy Res:2003 Jun-Jul;55(1-2):105-16. PMID: 12948620; doi.
Cell Studies & Basic Sciences
One of the early studies covering Holcomb’s work at Vanderbilt Medical University was a cell study. While only an in vitro study, it was important none-the-less because it demonstrated that different designs of static magnets can produce different physiological effects.
BASIC SCIENCES STUDY #1: EFFECTS OF MAGNETIC FIELDS ON ACTION POTENTIAL FIRING

Quadrapolar magnet blocking a nerves Action Potential firing
McLean et al. (1991). Effects of Steady Magnetic Fields on Action Potentials of Sensory Neurons in Vitro. Environ Med: 1991; 8 (2): 36 – 45.
This was a foundational study on the effects of static magnetic fields on sensory neurons, comparing the common bipolar magnets with multipolar magnets including the quadrapolar array. More specifically that Quadrapolar magnets will block action potential firing of a dorsal root ganglion, while the common bipolar magnet has no effect. The comparison below is described.
Okano et al., (2012). The Effects of Moderate-Intensity Gradient Static Magnetic Fields on Nerve Conduction. Bioelectromagnetics. 2012 Mar 16. PMID: 22430817; doi.
Markov M.S., (2009). What need to be known about the therapy with static magnetic fields. Environmentalist: (2009) 29:169–176. doi.
Colbert et al. (2008). Static Magnetic Field Therapy: Dosimetry Considerations. J Altern Complement Med: 2008; 14(5). PMID: 18532897; doi.
Engstrom et al. (2005). Devices for gradient static magnetic field exposure. Bioelectromagnetics:2005 May;26(4):336-40.PMID: 15832330; doi.
Engstrom et al. (2002). Effects of non-uniform static magnetic fields on the rate of myosin phosphorylation. Bioelectromagnetics: 2002 Sep;23(6):475-9. PMID 12210566; doi.
Cavapol et al. (1995). Measurement and analysis of static magnetic fields that block action potentials in cultured neurons. Bioelectromagnetics.1995;16(3):197-206. PMID: 7677796; doi.
“McLean et al. (1995). Blockade of sensory neuron action potentials by a static magnetic field in the 10 mT range. Bioelectromagnetics:1995;16(1):20-32. PMID: 7748200; doi.
McLean et al. (1991). Effects of Steady Magnetic Fields on Action Potentials of Sensory Neurons in Vitro. Environ Med: 1991; 8 (2): 36 – 45.
Download PDF
Laakso et al (2009). Static Magnets – What are they and what do they do? Brazilian Journal of Physiotherapy: 2009;13(1):10-23; doi.
Download PDF
Can also be downloaded from SciELO Brazil.
This is a good place to start. It takes an honest look at static magnets, evaluates much of the published research and describes and compares the common bipolar and quadrapolar magnets.
McLean et al. (2001). Static Magnetic Fields for the Treatment of Pain. Epilepsy & Behavior2: S74-S80 (2001).doi.
This is a critical review of published data that supports potential therapeutic use of static magnetic field–generating devices. In particular it investigates the dosimetry and physiologic effects of quadrapolar magnetic devices.
Colbert et al. (2009). Static Magnetic Field Therapy: A Critical Review of Treatment Parameters. Evid Based Complement Alternat Med 6(2): 133-139. PMID 18955243. doi.
Can also be downloaded from Evidence-based Complementary and Alternative Medicine.
This paper is essentially a call for engineers, physicists and clinicians to continue to work together to optimise static magnetic field dosage and treatment parameters for each clinical condition. It is also a response to the review by Pittler et al (see below) who reviewed
Pittler et al. (2007). Static magnets for reducing pain: systematic review and meta-analysis of randomized trials. CMAJ: 2007 Sep 25;177(7):736-42. PMID: 17893349; doi.
Can also be downloaded from Canadian Medical Association Journal
This is a classic case of conducting an investigation in an attempt to reinforce a preconceived position. In spite of all the available evidence (a fraction of which is available on this website), this article concludes that…”the evidence does not support the use of static magnets for pain relief, and such magnets therefore cannot be recommended as an effective treatment”.
Compare this paper’s summary of Segal et al (2001)– “No significant differences (to pain levels)” to that of Laakso et al (2009)– “Significantly less pain in treatment group compared to control group”. One would wonder if they were reading from the same paper. Read it yourself to form your own opinion.
Antal et al. (2009). Exposure to Inhomogeneous Static Magnetic Field Ceases Mechanical Allodynia in Neuropathic Pain in Mice. Bioelectromagnetics: 2009 Sep;30(6):438-45. PMID: 19405037; doi.
Inhomogeneous static magnetic field refers to a multipolar field gradient producing magnet as opposed to a simple bipolar homogenous magnetic field. The results suggest that exposure to iSMF cannot prevent the development of mechanical allodynia, but can inhibit processes that maintain the increased sensitivity to mechanical stimuli in neuropathic pain.
Laszlo et al. (2007). Optimization of static magnetic field parameters improves analgesic effect in mice. Bioelectromagnetics 2007 Dec;28(8):615-27. PMID: 17654477; doi.
Hungarian Academy of Science compares numerous static magnetic fields for their analgesic effect in mice. Finds that the gradient modulated array achieves an analgesic effect of over 80% in the writhing test. Conclusion: As a non-drug, non-invasive, non-contact, non-pain, non-addictive method for analgesia with immediate and long-lasting effect based on the stimulus of the endogenous opioid network, the static magnetic field treatment may attract the attention of medical doctors, nurses, magnet therapists, veterinarians, physiotherapists, masseurs, and fitness trainers among others.
Laszlo et al. (2009). 3 T homogeneous static magnetic field of a clinical MR significantly inhibits pain in mice. Life Sciences: 2009 Jan 2;84(1-2):12-7. PMID: 19000698; doi.
Can also be downloaded from ScienceDirect
This Hungarian study looked at antinociceptive activity in the writhing test in mice and concluded that a 3 Tesla homogeneous static magnetic field of a clinical magnetic resonance system induces a significant pain-inhibitory effect in the writhing test in mice. In this experiment, naloxone pretreatment reversed the pain-inhibitory effect of the static magnetic field confirming the hypothesis that an opioid component may be involved in the action.
Morris et al. (2008). Acute Exposure to a Moderate Strength Static Magnetic Field Reduces Edema Formation In Rats. Am J Physiol Heart Circ Physiol: 2008 Jan;294(1):H50-7. PMID: 17982018; doi.
Can also be downloaded from American Journal of Physiology – Heart and Circulatory Physiology
This study claims to be the first to demonstrate that acute, localized static magnetic field exposure of moderate field strength (5-100 mT), when applied immediately after an inflammatory injury, can result in significant reduction of edema formation. While the study doesn’t necessarily relate specifically to magnetic field gradients as they used bipolar magnets, it does a very good job at measuring the magnetic field dosage and treatment parameters and the results were significant. It would be interesting to compare results with a static magnetic field with a steep field gradient. There is also a take home message for users of magnetic therapy, as soon as you have an injury – apply your devices.
Morris et al (2007). Chronic static magnetic field exposure alters microvessel enlargement resulting from surgical intervention. J Appl Physiol : 2007 Aug;103(2):629-36. PMID: 17478604; doi.
This research looked at the effects of a localised static magnetic field on oedema after trauma in mice. The most significant reduction in arteriolar enlargement was manifested in the smallest vessels. As an example at day 7 sham treated vessels revealed venular enlargement of 91%, whereas magnet treated only 41%. This study blows away the common assumption that the healing of SMF’s in induced by increasing the blood flow to the injured area.
McLean et al. (2003. A static magnetic field modulates severity of audiogenic seizures and anticonvulsant effects of phenytoin in DBA/2 mice. Epilepsy Res:2003 Jun-Jul;55(1-2):105-16. PMID: 12948620. doi.
Okano et al., (2012). The Effects of Moderate-Intensity Gradient Static Magnetic Fields on Nerve Conduction. Bioelectromagnetics. 2012 Mar 16. PMID: 22430817; doi. Reference Article by Q Magnets
Nerve conduction velocity (NCV) was measured and compared within three groups, a control and a 0.21 Tesla and 0.7 Tesla iSMF. The researchers speculate that the action of moderate-intensity iSMF may act in a similar way to that of Na+ channel-blocking anaesthetics.
This article needs an applause:
Markov M.S., (2009). What need to be known about the therapy with static magnetic fields. Environmentalist: (2009) 29:169–176. doi.
Download PDF
Can also be downloaded from Springer Science.
In a critique of previous research, Marko Markov clearly articulates the inadequacies and describes what improvements need to be made if future research is to be credible and reproducible. It is also to a large degree a response to the study published in Anesthesia & Analgesia called Static Magnetic Therapy does not decrease pain or opioid requirements: A randomized double-blind trial.
Colbert et al. (2008) Static Magnetic Field Therapy: Dosimetry Considerations. J Altern Complement Med: 2008; 14(5). PMID: 18532897; doi.
Journal Link
A recent systematic review of SMF trials for pain reduction concluded that the evidence does not support the use of permanent magnets for pain relief. We argue that this conclusion is unwarranted if the SMF dosage was inadequate or inappropriate for the clinical condition treated.
Engstrom et al. (2005). Devices for gradient static magnetic field exposure. Bioelectromagnetics:2005 May;26(4):336-40. PMID: 15832330; doi.
Technical paper investigating dosimetry with field amplitude and gradient.
Engstrom et al. (2002. Effects of non-uniform static magnetic fields on the rate of myosin phosphorylation. Bioelectromagnetics: 2002 Sep;23(6):475-9. PMID 12210566; doi.
Download PDF
This study investigates the effect of static magnetic field gradients on the rate of myosin phosphorylation. Findings confirmed that the most biological active region of the quadrapolar magnet was at the boundary between the poles where the magnetic field gradient was steepest.
Cavapol et al. (1995). Measurement and analysis of static magnetic fields that block action potentials in cultured neurons. Bioelectromagnetics.1995;16(3):197-206. PMID: 7677796; doi.
Download PDF
Findings suggested that the magnetic field gradient and not strength of the field was determining factor in action potential blockade.
McLean et al. (1995) Blockade of sensory neuron action potentials by a static magnetic field in the 10 mT range. Bioelectromagnetics:1995;16(1):20-32. PMID: 7748200;
doi.
Download PDF
Articles on Magnet Therapy Research

How Static Magnetic Fields Are Shaping the Future of Organ Preservation
The medical world is no stranger to the potential of magnetic fields, particularly static magnetic fields (SMFs), which have been shown to positively impact human health and biological processes. A recent study published in Cell Reports Physical Science brings renewed...

Q Magnets Case Study Published in the Medical Acupuncture Journal
Medical acupuncturists are experts at identifying and accurately locating the morphological structures to be targeted. Quadrapolar, or Q Magnets produce an optimised field and provide the acupuncturist with an additional modality to target these structures that is...
Fan, Y et al (2021) research review on analgesic effects of static magnetic field therapy
An in-depth research review on the analgesic effects of static magnetic field therapy has just been published in Bioelectromagnetics. The journal is published by BEMS (the Bioelectromagnetic Society) and is the authoritative record for natural and applied...
Cellular Level Anti-Inflammatory Effects of Static Magnetic Fields
Read this research review article to learn how static magnetic fields work on a cellular level to reduce inflammation based on published clinical research.
Static magnetic fields enhancing stem cell activity
Stem cell research shows that static magnetic fields may enhance the body’s natural ability to stimulate dentine formation. Dentinogenesis can be facilitated through stem cell proliferation, migration and differentiation, which previous studies have shown can be improved with an external static magnetic field. Q Magnets such as our smallest QF10-2 can easily be applied to target gums and reduce pain. Read our research review to learn more.

Q Magnets: A possible Magneto-Neuromodulation Therapy?
Neuromodulation therapies apply a therapeutic stimulus directly to the nervous system. Ideally, neuromodulation techniques should be noninvasive, biocompatible, and spatially and temporally controllable. Examples of magneto-neuromodulation are Transcranial Magnetic...
Discovery of fibromyalgia biomarker offers hope of earlier diagnosis for sufferers
Fibromyalgia literally means 'fibrous muscle tissue pain', which is a pretty accurate description of the condition. Also referred to as 'Fibromyalgia Syndrome', or by the abbreviations 'FM' or 'FMS', sufferers experience the following symptoms... •...
People’s sensitivity to magnetic fields could differ, new research shows
We’ve known for some time that different people have different sensitivities to static magnetic fields. There doesn’t appear to be an obvious reason as to who, why or where, but as a health practitioner, you place magnets on enough patients and the differences in...
Clinical trial shows magnets provide pain relief from myofascial trigger points
The Physical Therapy department at Armstrong Atlantic State University conducted a Randomised Clinical Trial using static magnets on myofascial trigger point pain. The 2004 study was part of the student capstone project and supervised by professors of the physical...
Magnetic fields used in Transcranial Magnetic Stimulation (TMS)
SUMMARY: Transcranial Magnetic Stimulation (TMS) passes an unimpeded magnetic field through the scalp and skull. The action on the brain is caused by electromagnetic induction, which is basically creating electrical activity within a very specific part of the brain...

There is no comparison
Since 2009 Q Magnets have led the way with the world’s most effective magnetic therapy devices. We provide a 30-day satisfaction guarantee and deliver worldwide including Unites States, Canada, New Zealand, Europe & South East Asia.
We support our products with advice from experienced health professionals for device selection and placement to achieve the best results. Feel free to write to us anytime!