Central Sensitization
Central Sensitization is an increase in the excitability of neurons within the central nervous system starting at the spinal cord level. Normal inputs from everyday experiences such as touch are amplified to produce abnormally painful responses. Central Sensitization is a major cause of pain hypersensitivity.

Central Sensitization: When the Nervous System Amplifies Pain
Central sensitization is a condition in which the central nervous system becomes hypersensitive to sensory input, causing normal signals from the body to be interpreted as painful.
Instead of pain reflecting the severity of an injury, the nervous system itself becomes over-responsive, amplifying signals from the body.
This phenomenon is now recognised as one of the key biological mechanisms behind many forms of chronic pain.
In central sensitization:
• the spinal cord and brain become more excitable
• pain signals are amplified
• normal sensations such as touch can become painful
• pain may spread beyond the original injury
Central sensitization helps explain why pain can persist long after tissues have healed.
Central Sensitization and Chronic Pain
Central sensitization plays an important role in the pathophysiology of many chronic pain conditions, including:
• chronic low back pain
• fibromyalgia
• migraine
• post-herpetic neuralgia (shingles)
• diabetic neuropathy
• temporomandibular joint disorder (TMJ)
• complex regional pain syndrome (CRPS)
In these conditions, pain is no longer driven primarily by tissue damage but by changes in how the nervous system processes sensory signals.
Researchers now recognise that chronic pain often develops through a progressive cascade of nervous system changes, beginning with local tissue injury and potentially evolving into central nervous system hypersensitivity.
To understand this broader process, see our article:
Why Pain Becomes Chronic And Why Early Treatment Matters
Central Sensitization can also be a consequence of dysfunctional pain processing such as fibromyalgia, where somehow normal neural inputs from mechanotransducers get diverted into the pain pathway.
The underlying mechanisms of Central Sensitization are complex and not fully understood. They are thought to involve neurotransmitters such as glutamate and substance P that cause nerve fibres to become more “leaky” to Na+ and Ca2+ ions and hence lower the neural activation threshold.
Peripheral Sensitization and Ion Channel Proliferation
Modern pain neuroscience has also identified important changes that occur before central sensitization develops, particularly at the level of the peripheral nerves.
Research discussed in the Explain Pain framework developed by David Butler and the Neuro Orthopaedic Institute (NOI Group) describes how injured nerves undergo adaptive changes that increase their sensitivity.
One of the most important of these changes is ion channel proliferation.
Following tissue injury or nerve irritation, the body may increase the number of ion channels — particularly sodium channels — located on the cell membrane of sensory neurons.
This process may begin within days of injury and can continue for several weeks.
These additional ion channels create areas of increased electrical sensitivity along the nerve fibre.
Researchers sometimes describe these areas as abnormal impulse generating sites (AIGS).
Because ion channels control the movement of electrically charged ions across the nerve membrane, increasing their density makes the nerve easier to activate.
In practical terms, this means:
• the threshold for firing a pain signal becomes lower
• neurons become more excitable
• spontaneous nerve firing may occur
This process is commonly referred to as peripheral sensitization.
The Sensitization Cascade
These changes can be viewed as part of a broader sensitization cascade:

As the density of ion channels increases on the nerve membrane, the nervous system becomes progressively more responsive to stimulation.
If these signals continue to bombard the spinal cord, neurons within the dorsal horn may also become more excitable, leading to central sensitization.
Ca2+ ions also initiate a range of intracellular signalling cascades that lead to the production of prostaglandins that further lowers the threshold for neuronal activation within the dorsal horn. The sensitization of these neurons means that they can now be stimulated by formally innocuous stimuli (allodynia), in addition, these neurones can produce an exaggerated response to noxious stimuli (primary hyperalgesia) and spread the sensitivity to non-injured areas (secondary hyperalgesia).
What Happens at the Cell Membrane
At the microscopic level, this process can be summarized as:

These changes represent a form of neuroplasticity, meaning the nervous system adapts to injury.
Importantly, modern pain neuroscience emphasizes that these changes are dynamic and reversible.
When the drivers of sensitization are reduced, nerve excitability may gradually return toward normal levels.
Recognising Central Sensitization in Clinical Practice
Clinicians often recognise central sensitization through several key features.
Hyperalgesia
Painful stimuli produce greater than normal pain responses.
For example, a mild injury may cause disproportionate pain.
Allodynia
Normally non-painful sensations become painful.
Examples include:
• light touch
• clothing brushing the skin
• gentle pressure
Secondary Hyperalgesia
Pain sensitivity spreads to areas surrounding the original injury, even where tissue damage has not occurred.
Persistent Pain
Pain continues long after tissue healing should have occurred.
(Nijs, Van Houdenhove et al. 2010) provided guidelines for manual therapists to recognise central sensitization in patients with musculoskeletal pain. The examination included for instance…
1. Assessment of pressure pain thresholds at sites remote from the symptomatic site;
2. Assessment of sensitivity to touch during manual palpation at sites remote from the symptomatic site; and
3. Assessment of pressure pain thresholds during and following exercise
(Nijs, Meeus et al. 2011) provided a list of treatment options for the treatment of central sensitization, which included pharmacotherapy such as acetaminophen (paracetamol), serotonin-reuptake inhibitor drugs, opioids, NMDA receptor blockers and Ca2+ channel ligands such as pregabalin and gabapentin.
Just like context-dependant drugs, biological studies and clinical experience shows that Q Magnets appear to work in a similar way in that they only effect “pathological” pain transmission and not “normal” pain transmission and without the side-effects.
In their list of treatment options for central sensitization, (Nijs, Meeus et al. 2011) also included repetitive transcranial magnetic stimulation, which has short term analgesic effects, TENS, manual therapy, neurofeedback and cranial electrotherapy stimulation.
Magnetic Field Gradients and Nerve Excitability
Research over several decades has suggested that inhomogeneous static magnetic fields may influence nerve activity.
Laboratory studies conducted by neurologists at Vanderbilt University investigated the effects of magnetic field gradients on sensory neurons.
These studies demonstrated that exposure to specific static magnetic fields could alter neuronal excitability by affecting membrane permeability to sodium and calcium ions.
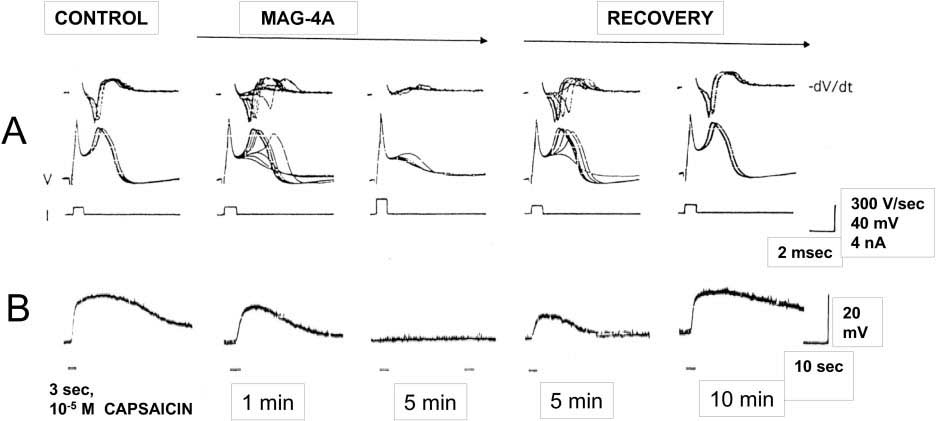
In one experiment, cultured sensory neurons exposed to capsaicin (a noxious stimulus) showed sustained firing of action potentials. When exposed to a steep magnetic field gradient generated by a quadrapolar magnet array, neuronal firing was temporarily blocked and later returned to normal once the field was removed.
These findings suggest that magnetic field gradients may influence neural signalling involved in pain transmission.
Magnetic Therapy and Targeted Neuromodulation
Unlike systemic pharmacological treatments, magnetic therapy devices are typically applied locally over specific anatomical targets.
One advantage of wearable magnetic devices is that they can provide continuous exposure to the therapeutic field without interfering with normal daily activities.
In clinical practice, magnetic devices are sometimes placed:
• directly over painful tissues
• over spinal segments associated with the affected nerves
• over trigger points or sensitized regions
Correct device design and placement are critical, as the therapeutic effect depends on the characteristics of the magnetic field gradient reaching the target tissue.
Clinical Observations
Clinicians working with patients experiencing chronic pain have reported that when magnetic field therapy is correctly applied, some patients experience noticeable reductions in pain sensitivity.
In certain cases, improvements have included:
• decreased hypersensitivity to touch
• improved tolerance to movement or manual therapy
• reductions in background pain levels
While these observations require further scientific investigation, the low risk associated with non-invasive magnetic therapy makes it an area of ongoing clinical interest.
After 10 years of research including in-vitro cell studies and randomised controlled trials the group of neurologists at Vanderbilt Medical University lead by Dr Robert Holcomb, M.D., Ph.D. concluded that the evidence suggested that the most likely mechanism of action is that the steep field gradients generated by the quadrapolar magnetic field is altering nerve excitability as a result of changes in membrane permeability to Na+ and Ca2+ ions (McLean, Holcomb et al. 1991), (McLean, Holcomb et al. 1995), (Cavopol, Wamil et al. 1995), (McLean, Engstrom et al. 2001).
(McLean, Engstrom et al. 2001) describes the cell study where nerve fibres were exposed to the noxious stimuli capsaicin and after 5 minutes of exposure to the gradient of the Quadrapolar array, the action potential firing was totally blocked and fully recovered 10 minutes after the removal of the field.
In a double blind, randomised controlled trial (Vallbona, Hazlewood et al. 1997) assessed the effectiveness of a concentric alternating multipolar rubberised magnet which produces a magnetic field gradient, albeit most likely with a penetration of less than 5 mm. Of the 50 post-polio patients enrolled in the study, 29 were in the active group and 21 the inactive. The devices were placed over the most painful trigger point for 45 minutes. Those who received the active device reported significantly less pain than those that received the sham device.
As an indication of the therapeutic effects of an inhomogeneous static magnetic field on peripheral sensitization, Kovacs-Balint et al (2011) conducted a double-blind, placebo controlled trial and demonstrated that exposure to an optimized field significantly increased the thermal pain threshold in healthy young adults.
What is clear when it comes to magnetic therapy is that unless you are using a magnetic device with an optimised design, with the right field characteristics, correctly placed so that the penetrating field envelopes the offending target tissue, then the therapy is unlikely to be effective.
With the recent release of the third generation Q Magnet models it is now possible to apply a device with an optimised therapeutic field that will envelope the target tissue. Specifically when it comes to central sensitization, the most important devices for the lumbar spine are QF28-6 and QF28-3 and where there are two adjacent levels indicated, usually L4/5 and L5/S1 the OF50-3. The OF50-3 model is a powerful rare earth neodymium octapolar magnet with a 50mm diameter that can envelope adjacent levels of the spinal cord with a magnetic field gradient, which to our knowledge is the first time this has been achieved with a static magnet device.
What is encouraging for practitioners working with complex chronic pain conditions is that clinical observations suggest that when Q magnet therapy is correctly applied, reductions in hypersensitivity and improvements in symptoms may sometimes occur quite rapidly.
While the scientific evidence for these observations requires much more research, the advantage for the patient is that the risk of intervention and expense is almost negligible.
Understanding the Bigger Picture of Chronic Pain

Central sensitization is only one stage within a broader process through which pain can become chronic.
Researchers now describe a pain chronification cascade in which:
- Tissue injury triggers peripheral sensitization, partly driven by ion channel proliferation on nerve membranes.
- Persistent peripheral signals may then lead to central sensitization within the spinal cord.
- Over time, brain networks involved in pain processing can also reorganize, further reinforcing chronic pain.
Understanding these stages helps explain why early treatment of pain and injury is important.
To learn more about this broader framework, read:
Why Pain Becomes Chronic And Why Early Treatment Matters
Case Studies that demonstrate the effects of Q magnet therapy on Central Sensitization.
CASE STUDY 1 – By Lifestyle Therapies in Brisbane, Australia
Sam, a fifty year old man with a 15 year history of chronic lower back pain was referred to Lifestyle Therapies from a local health provider. Sam had been suffering with constant deep pain and numbness in his right foot for 15 years, initially injuring his back when he was 20 years old. In his thirties, Sam underwent a laminectomy, followed by lumbar fusion of L5-S1 a few years later. Since then he has not lived a day without pain, significantly affecting his quality of life. In addition Sam was suffering hyperalgesia in his lower back due to an incident with a TENS machine. His skin in the lumbar spine was so sensitive, wearing clothes was unbearable which was an indication of Central Sensitization. He was unable to sit in a car for more than one hour without suffering significantly. Sam had one goal, which was to return to his hobby of painting.
- Initial assessment findings:
- Muscle inhibition of core muscles
- High tones in gluteal muscles
- Tender to touch adductors, ITB, and Quadricep muscles.
The lumbar region was hypersensitive to pain, even with light touch; a sign of static mechanical allodynia.
Sam was fitted with the OF50-3 Octapolar Q Magnet. This neuromagnetic device was selected since it’s large enough to cover the adjoining lumbar vertebrae L4/5 and L5/S1.
One week after seeing Sam, he reported having pain-free moments for the first time in 14 years. He was also able to tolerate the drive from his house to the clinic with minimal pain. During the next week Sam was disappointed that his symptoms were returning. After examining the Q Magnet, he realised it had been reattached incorrectly, with the sticker and flux plate facing the skin. Once corrected, his symptoms immediately began to subside.
After seven sessions, Sam’s hypersensitivity had dropped significantly and was able to sit and paint for 5 hours. He had no pain with touch, showing central desensitisation.
Since being able to enjoy pain free moments and tolerating hands on treatment such as massage, Sam has significantly improved his quality of life.
CASE STUDY 2 – By Edwards Physiotherapy in Auckland, New Zealand
JC is a medical doctor and had sufferred with chronic backache for about 14 years with varying degrees of pain and stiffness, with pins and needles. When the pain was particularly bad, JC would feel lethargic and down, and have difficulty sleeping and have to take pain-killers to find some relief. JC tried all sorts of treatment: physiotherapy, chiropractic, osteopathy, neurolink, Chinese and Western acupuncture, breathing exercises, etc. Most forms of treatment would only give me temporary relief.
JC was referred to Edwards Physiotherapy and was introduced to Q Magnets. JC felt much less pain in just 15 minutes after the QF28-3 was applied and improved again when the OF50-3 was applied. For the first time in over a decade, JC can go through her day feeling quite comfortable while wearing the OF50-3. JC now responds well to the Feldenkrais treatment, which she had been seeking in the previous two years and is hopeful that one day she will be completely healed.
REFERENCES:
Butler, D., Moseley, L. (2003). Explain Pain. Adelaide, Australia: Neuro Orthopaedic Institute (NOI Group).
Cavopol, A. V., A. W. Wamil, et al. (1995). “Measurement and analysis of static magnetic fields that block action potentials in cultured neurons.” Bioelectromagnetics 16(3): 197-206.
Kovacs-Balint, Z., A. Csatho, et al. (2011). “Exposure to an inhomogeneous static magnetic field increases thermal pain threshold in healthy human volunteers.” Bioelectromagnetics 32(2): 131-139.
Lyndon, S. (2026). Pathophysiology of Chronic Pain. Clin J Pain. doi:10.1097/AJP.0000000000001362. PMID: 41614224.
McLean, M., S. Engstrom, et al. (2001). “Static Magnetic Fields for the Treatment of Pain.” Epilepsy & Behavior 2(3): S74-S80
McLean, M. J., R. R. Holcomb, et al. (1991). “Effects of Steady Magnetic Fields on Action Potentials of Sensory Neurons in Vitro.” Environmentalist 8(2).
McLean, M. J., R. R. Holcomb, et al. (1995). “Blockade of sensory neuron action potentials by a static magnetic field in the 10 mT range.” Bioelectromagnetics 16(1): 20-32.
Nijs, J., M. Meeus, et al. (2011). “Treatment of central sensitization in patients with ‘unexplained’ chronic pain: what options do we have?” Expert Opin Pharmacother 12(7): 1087-1098.
Nijs, J., B. Van Houdenhove, et al. (2010). “Recognition of central sensitization in patients with musculoskeletal pain: Application of pain neurophysiology in manual therapy practice.” Man Ther 15(2): 135-141.
Vallbona, C., C. F. Hazlewood, et al. (1997). “Response of pain to static magnetic fields in postpolio patients: a double-blind pilot study.” Arch Phys Med Rehabil 78(11): 1200-1203.
FAQs
Frequently Asked Questions About Central Sensitization
What is central sensitization?
Central sensitization is a condition in which the central nervous system becomes hypersensitive to sensory signals.
Instead of pain reflecting the severity of a tissue injury, the spinal cord and brain begin amplifying incoming sensory information.
As a result, normal stimuli may be perceived as painful, and painful stimuli may feel more intense than expected.
Central sensitization is now recognised as a key mechanism involved in many forms of chronic pain.
What causes central sensitization?
Central sensitization usually develops after persistent or repeated activation of pain pathways.
Common triggers include:
• injury or tissue inflammation
• nerve irritation or damage
• ongoing musculoskeletal strain
• repeated painful stimulation
When these signals continue over time, neurons in the spinal cord and brain can become more excitable.
What is peripheral sensitization?
Peripheral sensitization refers to increased sensitivity of nerves near the site of an injury.
Following tissue damage, inflammatory chemicals and cellular changes can make sensory nerves more responsive to stimulation.
One important mechanism involves ion channel proliferation on the nerve cell membrane, particularly sodium channels.
What is hyperalgesia?
Hyperalgesia is a condition in which painful stimuli produce a stronger-than-normal pain response.
What is allodynia?
Allodynia occurs when normally non-painful sensations become painful.
Examples include:
• light touch
• clothing brushing against the body
• gentle pressure
Can central sensitization be reversed?
In many cases, central sensitization can improve over time because the nervous system is capable of neuroplastic change.
Treatment approaches may include:
• pain neuroscience education
• graded movement or exercise
• cognitive behavioural strategies
• neuromodulation therapies
• appropriate medical management
-
 Q Bonus Package - General UseUS$209.00
Q Bonus Package - General UseUS$209.00 -
 Q Bonus Package - Complex Lower Back PainUS$384.00
Q Bonus Package - Complex Lower Back PainUS$384.00 -
 Q Bonus Package - Lower Back PainUS$246.00
Q Bonus Package - Lower Back PainUS$246.00 -
 Q Bonus Package - Active AthleteUS$487.00
Q Bonus Package - Active AthleteUS$487.00 -
 Q13 Blanket (Sm)US$530.00
Q13 Blanket (Sm)US$530.00

Got Q Magnets ?
We are dedicated to support our products with sound advice from experienced health professionals to achieve the best results!